Biomedical Engineering: A Literature Review
Introduction
Biomedical Engineering has seen a subsequent growth in the health care industry over the past 40 years. However, research and innovations in this field have surged in recent years amid the advancement in learning sciences. To meet the current needs of ever-growing health care infrastructure there is a dire need for designing new reforms and learning new systems and technology in engineering education. This article provides an insight into the education related to Biomedical Engineering and an approach to enhance the conventional systems and optimize the current learning opportunities for biomedical engineering.
What is Biomedical Engineering?
As per the Biomedical Engineering Society, the Biomedical Engineer as an expert to investigate and resolve problems on biology and medicine by application of sophisticated technology to the complex issues of medical care. Biomedical Engineers teams up with health care professionals to design devices, instruments, and software, besides, to bring together knowledge from technical sources to develop new procedures and get to the bottom of clinical issues (Harris, 2003).
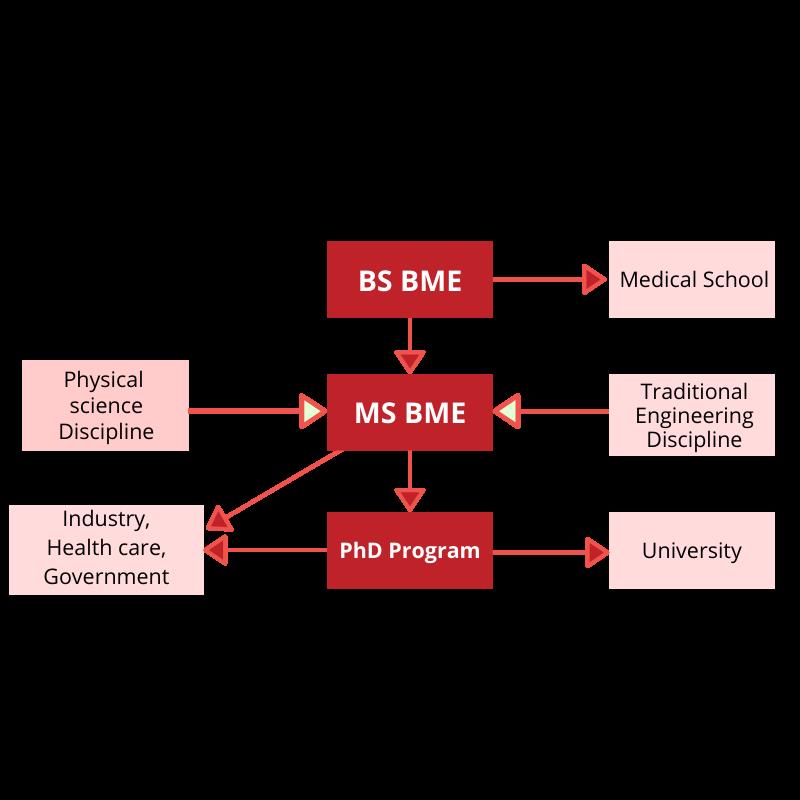
In other definitions, Biomedical Engineering integrates the clinical practices and biomedical sciences with the engineering sciences by knowledge acquisition and understanding living organisms through analytical and experimental techniques. It enhances the overall health care and medical practice by the development of algorithms, processes, devices, and systems. The figure below explains the scope of BME.
Evolution of Biomedical Engineering
Biomedical Engineering is progressing in leading academic institutions around the globe. IEEE Transactions in Biomedical Engineering (1975) made a special attempt under its special issue in which various topics including the founding of BME, educational approaches, engineering in health care, and biomedical engineer’s role in the healthcare industry were discussed. The discussions were based on monitoring and instrumentation devices, ultrasound, bio-fluid mechanism, quantitative physiology, and clinical engineering (Tatroe & Blanchard, 1999).
Whitaker Foundation (2020) organized an international summit on BME education. The meeting produced major data that indicated the constant growth of the enrollment in BME education. It was observed that substantial biomedical service has arisen providing opportunities to BME graduates. In 2005, the foundation sponsored another summit for designing the programs to help universities modify their existing structure of Biomedical Engineering to meet future requirements. These summits have laid the foundation for the modern-day BME research. There have been subsequently numerous curricular reforms by The National Science Foundation for the development of engineering education. Special emphasis on the training of students for the practice of Biomedical Engineering in industries and health care organization was laid. The R&D in the field of BME is evolving till date for better assistance of engineering studies to the medical sciences (Abu-Faraj, 2008).
Relevant Sciences to BME
BME is itself a vast field of learning combining the medical and engineering sciences. An extremely essential trait of expertise is the capability to smoothly distinguish and deduce significant patterns of information. A conditionalized knowledge is vital for the expertise which is obtained by modern problem-solving processes. The enhancement in case, project, and problem-based learning have been an approach to solve issues occurring in domains of BME. These methods have been conventionally used in business and law schools, and other areas of engineering, science, and mathematics. Knowledge-centered learning and qualitative thinking by organizing key concepts are positive designs for learning environments. The students should be able to make their thinking visible for community-centered approach (Harris, Bransford, & Brophy, 2002)
Role of Technology in BME
New technologies create feasibility to employ insight from learning theories to improve both the student as well as faculty learning. The authentic and difficult cases applicable to biology, medicine, mathematics relating to BME can be searched and explored using technology. Simulated environments can give students hands-on training on realistic situations and in-depth knowledge can be gained about the subject. Electronic references are more convenient from the text-based resources in terms of search and update. Online conferences facilitate the flow of knowledge from different geographical locations. Software like MATLAB and CAD can help in mathematical modeling and visualizations in BME. Technology has played an important role in communication and community building of the students and faculties from different continents.
Key Areas of Biomedical Engineering
The elements of crucial knowledge for efficient practice include skills and techniques, development of skills, and educational strategies for the communication of knowledge (Biomedical Engineering Society, 1996). As per the Whitaker foundation, here are the key areas of the BME.
Basic
- Biomechanics
- Bioinstrumentation
- Biosystems
- Cell/molecular Engineering
- Biomaterials
Advanced
- Functional genomics
- Biomems (bio-micro-electro-mechanical systems)
- Cell/tissue engineering
- Computational Biology
- Bioimaging
Challenges in the development of BME
Biomedical engineering has to offer students practical information in both engineering and biology in 4 years which is difficult to be attained as the two subjects are very comprehensive on their own. Thus, there is an obligation of effectiveness for providing students with an understanding of both the fields as both the engineering and biology are developing separately at speedy rates. Enhanced learning at all levels can assist to rise above this barrier. The general separation of industry and immaturity of academic work in certain aspects is another barrier. Extensive academic research to address the issues of the industry can help the students and institutions to realize the potential of Biomedical Engineering. Closer contact of engineering students with health care and clinical science can bridge this gap.
Conclusion
As per the U.S. Department of Labor (DOL, Washington, DC, USA), there will be an overwhelming growth in the BME and it is very unlikely that BME will become saturated. A subsequent surge in the number of students enrolling in this field was seen as well (Simon, 1980). There are various domains for Biomedical students such as product design and development, research, data processing, sales and marketing, general and technical design, consulting, quality-related, patenting assignments, purchasing assignments, financial administration, production management, and planning, and many more. Students can undergo a master’s degree in Business to manage or run a healthcare organization or Doctoral degree in BME that can open up numerous pathways for the aspirant in this field.
References
- Abu-Faraj, Z. O. (2008). Bioengineering/biomedical engineering education and career development: literature review, definitions, and constructive recommendations. International Journal of Engineering Education, 24(5), 990.
- Biomedical Engineering Society. (1996). Planning a Career in Biomedical Engineering.
- Harris, T. R. (2003). Recent advances and directions in biomedical engineering education. IEEE Engineering in Medicine and Biology Magazine, 22(4), 30–31.
- Harris, T. R., Bransford, J. D., & Brophy, S. P. (2002). Roles for learning sciences and learning technologies in biomedical engineering education: A review of recent advances. Annual Review of Biomedical Engineering, 4(1), 29–48.
- Simon, H. A. (1980). “Problem Solving and Education” In Problem Solving and Education: Issues in Teaching and Research, ed. David T. Tuma and Frederic Reif, 81�96. Hillsdale, NJ: Erlbaum.
- Tatroe, & Blanchard. (1999). Electrical and electronics engineering.
- Whitaker. (2020). Conclusion of the Whitaker Program.
 Previous Post
Previous Post Next Post
Next Post